
Pain assessment is a fundamental aspect of healthcare. It allows not only for a better understanding of patients' suffering, but also for its effective management. The use of pain scales provides a systematic and validated method for quantifying and qualifying this experience, which remains deeply subjective.
These scales play an indispensable role for healthcare professionals. They allow for the precise identification of pain intensity, whether acute, prolonged, or chronic, and for adapting treatments accordingly. In this article, we will examine the importance of these tools, the different types of scales available, their practical use, and their integration into patient care. This includes specific cases such as those of children, the elderly, and individuals with verbal communication disorders.
Importance of Pain Assessment in Patients
Consequences of Untreated Pain
Untreated or inadequately relieved pain can have devastating consequences for patients' health and well-being. It can lead to psychological disorders such as depression and anxiety, disrupting almost all daily activities.
Patients with chronic pain may become inactive, withdraw from society, and focus exclusively on their physical health. This leads to significant loss of function and substantial disability. Furthermore, chronic pain can cause autonomic disorders such as fatigue, sleep disturbances, anorexia, and decreased libido, thus affecting the patient's overall quality of life. The economic costs of chronic pain are also considerable. For example, in Canada, the costs associated with lost workdays, medications, and medical consultations are estimated at approximately $10 billion annually. Impact on Quality of Life and the Healing Process: Proper pain assessment and treatment are essential to maintaining and improving patients' quality of life. Poorly managed pain can slow the healing process and increase the risk of postoperative complications, particularly after surgery. Furthermore, uncontrolled acute pain can develop into chronic pain, further complicating management and significantly reducing the patient's quality of life. A holistic approach, including medication and non-pharmacological techniques such as rehabilitation, electrical stimulation, and manual therapy, is often necessary for effective pain management. This underscores the importance of an accurate pain assessment to tailor treatments to each patient's specific needs. Such an approach not only improves their quality of life, but also their healing process.
Understanding Pain Scales
Definition and Purpose of the Scales
Pain scales are systematic tools Designed to identify, quantify, and qualify the pain experienced by patients. Their primary objective is to provide an objective and reproducible measure of pain intensity, thus enabling healthcare professionals to diagnose, treat, and monitor the effectiveness of pain interventions.
These scales play a vital role in harmonizing care practices, optimizing pain monitoring, and ensuring reliable traceability of treatments.
Types of Pain Scales
There are several types of pain scales, each with its own specific characteristics and uses.
Numerical Rating Scale (NRS)
The Numerical Rating Scale (NRS) is one of the simplest and most commonly used methods. It involves asking the patient to rate their pain on a scale of 0 to 10, where 0 represents no pain and 10 represents the worst pain imaginable. This scale is easy to understand and use, and it is applicable to the majority of patients.
Visual Analog Scale (VAS)
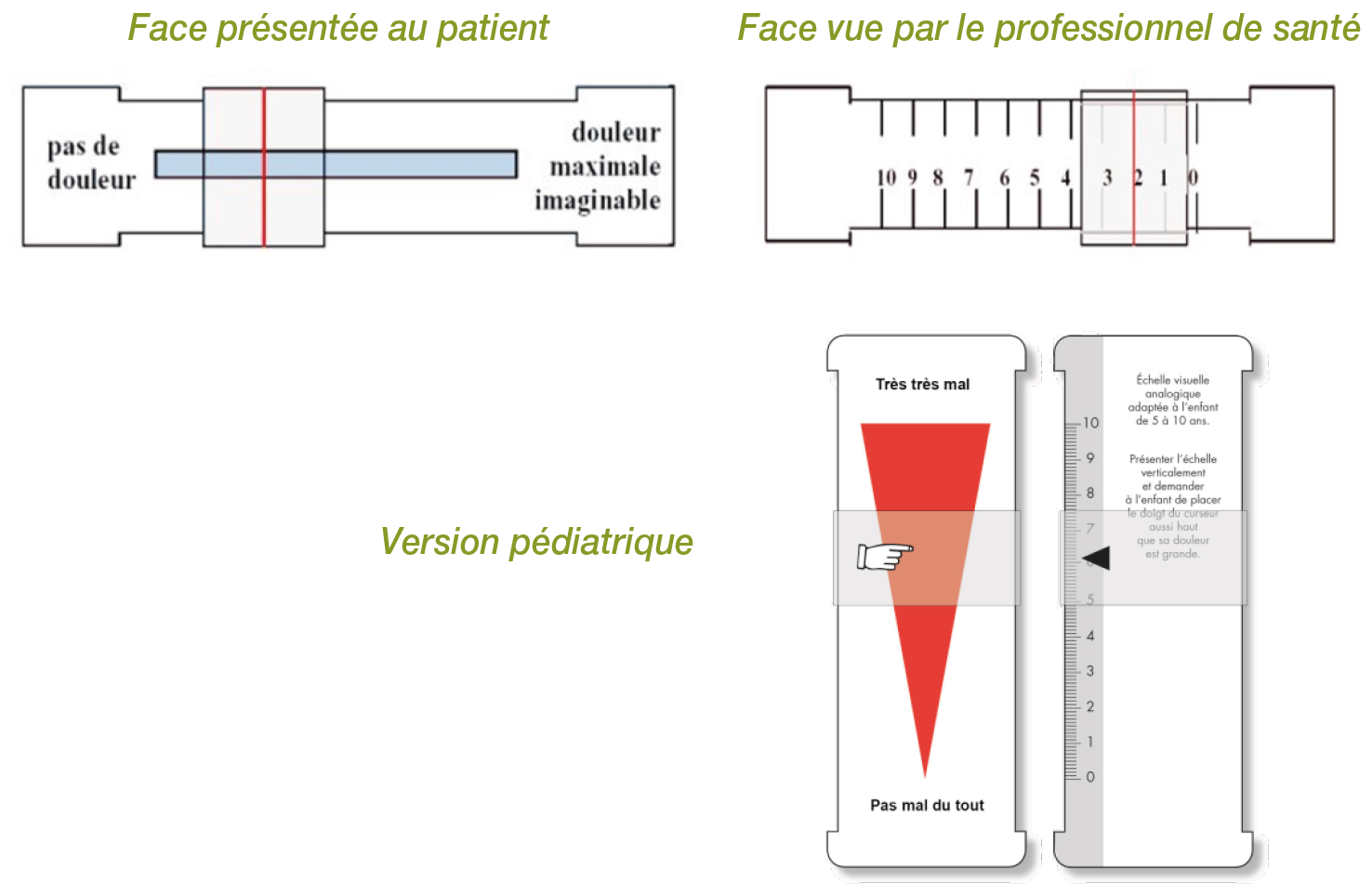
The Visual Analog Scale (VAS) is presented in the form of a graduated ruler or a 10 cm line. The patient positions a cursor or marks a point on the line to indicate their pain level, ranging from 0 (no pain) to 100 mm (unbearable pain).
This scale is particularly useful for patients who have difficulty with verbal adjectives or for those who do not speak the dominant language of the country.
Simple Verbal Scale (SVS)
The Simple Verbal Scale (SVS) is based on a series of adjectives to describe pain, such as "no pain, "mild pain, "moderate pain, "intense pain, and "intense pain. id="">"extremely intense". These adjectives are then transformed into numerical values ranging from 0 to 4. Easy to understand and use, this scale nevertheless has one limitation: individual variations in the perception of verbal terms.
These different scales offer the possibility of choosing the tool best suited to the patient, taking into account their communication abilities and their specific situation.
Pain Self-Assessment Scales

Visual Analog Scale (VAS)
The Visual Analog Scale (VAS) is one of the most reliable and widely used methods for self-assessment of pain. It takes the form of a straight line 100 mm long, with "no pain" marked at one end and "unbearable pain" at the other. The patient places a mark on this line to indicate the intensity of their pain at a given time. This scale is simple, reproducible, and sensitive to variations in pain intensity. Developed by Huskisson in 1974, it is particularly valued for its ease of use and reliability. The Numerical Rating Scale (NRS) is another commonly used method for self-assessing pain. It involves asking the patient to rate their pain on a scale of 0 to 10, where 0 represents no pain and 10 the worst pain imaginable. Easy to understand and use, this scale is a practical tool for both caregivers and patients. It is particularly well-suited to situations of acute or postoperative pain, where a rapid assessment is necessary. The Simple Verbal Rating Scale (SVR) offers a series of ranked descriptors to describe the intensity of pain. Patients can choose from terms such as "no pain," "mild pain," "moderate pain," and "severe pain."
This scale is often more accessible to patients who have difficulty with abstract concepts or who prefer verbal descriptions. It is also useful for a qualitative assessment of pain.
Hetero-Assessment Pain Scales
Face Legs Activity Cry Consolability (FLACC)
The FLACC scale, which stands for Face, Legs, Activity, Cry, Consolability, is a behavioral measurement tool designed to assess pain in children aged 2 months to 7 years, as well as in individuals unable to communicate their pain, including intubated adults in intensive care units (ICUs). This scale is based on the assessment of five specific criteria:
- Facial Expression: A normal expression or a smile (score 0), an occasional grimace or frown (score 1), or a constant trembling of the chin and a clenched jaw (score 2).
- Legs: Normal or relaxed position (score 0), restless or tense (score 1), or flapping or folded (score 2).
- Activity: Calm and in a normal position (score 0), restless or twisting (score 1), or arched, rigid, or startling (score 2).
- Crying: No crying (score 0), Occasional moaning or complaining (score 1), or constant crying, screaming, or sobbing (score 2).
- Consolability: Calm and relaxed (score 0), reassured by occasional contact (score 1), or difficult to console (score 2).
Each criterion is scored from 0 to 2, resulting in a total score from 0 to 10. This scale is particularly useful in situations where self-assessment of pain is impossible. It is an essential tool for caregivers to better understand and manage pain.
Neonatal Pain and Discomfort Scale (EDIN)
The Neonatal Pain and Discomfort Scale (EDIN) is specifically developed to assess pain in newborns. It relies on an analysis of several behavioral and physiological parameters to determine the level of pain experienced. The criteria assessed include: Facial expression, arm and leg movements, breathing, and level of alertness. Each criterion is scored according to a specific scale, and the scores obtained are combined to calculate an overall score that reflects the intensity of the pain. The EDIN is particularly useful in neonatal care units where newborns, unable to communicate their pain verbally, require special attention. This tool allows caregivers to effectively identify and manage pain in these vulnerable patients.
Pain Assessment in Specific Populations

Children and Pain Assessment
Pain assessment in children presents
From the age of 6, children are generally able to use more complex self-assessment scales, such as the Visual Analogue Scale (VAS) or the Numerical Rating Scale (NRS). These tools allow them to quantify their pain more precisely and independently.
Pain Assessment in Older Adults and Non-Communicative Individuals
Pain assessment in older adults, particularly those who are non-communicative or suffer from verbal communication disorders, requires specific approaches. In these situations, hetero-assessment scales are often the most appropriate. Although originally designed for newborns, the Newborn Pain and Discomfort Scale (NDDS) can serve as a model for assessing pain in non-communicative older adults. However, there are more specific tools adapted to this population. For example, the Behavioral Pain Scale (BPS) assesses pain through observable behaviors, such as facial expressions, limb movements, and vocalizations. This method is valuable for detecting and measuring pain in individuals unable to express it verbally. It is essential to consider the individual characteristics of each patient, including their medical history, cognitive status, and communication abilities. By adapting the pain scale to their specific needs, we ensure an accurate assessment and appropriate management of their pain.
Integration of pain scales into patient care
Training healthcare staff in the use of scales
Training healthcare staff is essential to ensure the effective and consistent use of pain scales. Healthcare professionals must be well-informed and trained on the different scales available, their advantages and limitations, and how to use them appropriately.
This training includes both theoretical knowledge of the scales and clinical practices for concrete and effective application.
It is important to raise awareness among healthcare teams of the importance of pain assessment and the need to integrate it into daily care routines, just like measuring pulse, blood pressure, and temperature. The designation of specifically trained pain specialists can also be implemented to provide appropriate responses and ensure consistency in the pain management strategy.
Role of Pain Scales in Optimizing Treatment
Pain scales play a central role in optimizing treatment. They allow for the quantification and qualification of pain, which is essential for tailoring treatments to each patient's specific needs. By asking patients to rate their current pain, as well as their worst and worst pain over the past 24 hours, healthcare professionals can gain a comprehensive view of pain progression. This allows them to adapt treatments accordingly. The use of pain scales is also a valuable tool for monitoring the effectiveness of treatments and making adjustments as needed. For example, if a patient reports an increase in pain despite treatment, healthcare professionals can review the treatment strategy and modify medications or interventions to improve pain control. This collaborative approach between the patient and the healthcare team is essential for optimal care. In addition, pain scales make it possible to determine the intervention threshold, that is, the level of pain from which specific actions must be taken to relieve the patient. This helps maintain an acceptable level of pain and significantly improves patients' quality of life.
Challenges and limitations of current pain scales

Limitations of self-assessment scales
Self-assessment pain scales, Although useful, these tools have significant limitations that can affect their reliability and effectiveness. One of the main difficulties lies in the understanding and use of these tools by some patients. For example, the elderly or those with cognitive impairments may have difficulty establishing a relationship between a numerical rating and the intensity of their pain, particularly with numerical rating scales. Furthermore, there is a risk of underestimating or overestimating pain due to various factors. Some patients underestimate their pain for fear of bothering caregivers or because of prejudice. Conversely, conditions such as anxiety, hypochondria, or hysteria can lead to overestimation. Older adults, in particular, often tend to assess the functional consequences of their pain rather than its intensity, which can skew the results. Sensory impairments, altered consciousness, coma, aphasia, dementia, and behavioral disorders all complicate the use of self-assessment tools. Even the simple verbal scale, often considered the most suitable in geriatrics, is not immune to these limitations. The search for better assessment methods: Faced with these limitations, it is imperative to continue innovating and developing more effective assessment methods. Technological advances and a better understanding of pain offer promising prospects. For example, artificial intelligence and machine learning could be used to analyze facial expressions and behavioral cues for a more objective assessment, particularly in non-communicative patients. Furthermore, combining multiple scales and assessment methods could improve the reliability of the results. For example, the combined use of the Visual Analogue Scale (VAS), the Numerical Rating Scale (NRS), and the Verbal Rating Scale (VRS) could provide a more comprehensive view of the intensity of pain experienced. This multimodal approach would overcome the limitations inherent in each scale while providing a more comprehensive assessment. Ongoing research in this area is essential to design pain assessment tools that are more sensitive, more specific, and better suited to the diverse needs of patients, regardless of their age or health status. Conclusion: Pain assessment plays an important role in healthcare, allowing for the quantification and effective management of patient suffering. Pain scales, whether self-assessed or assessed by others, are essential tools for healthcare professionals. It is crucial to choose the most appropriate scale for the patient, taking into account their age, health status, and communication abilities. Furthermore, training healthcare staff in the use of these tools is essential to ensure accurate assessment and optimal pain management. The limitations of current scales must be acknowledged, and further research is needed to develop new, more reliable and precise assessment methods. By systematically integrating pain assessment into care routines, we can significantly improve patients' quality of life and optimize their treatment. It is imperative to take action by adopting these practices in healthcare facilities to provide more personalized and effective care.
FAQ
What are the pain scales?
The main pain scales include:
- Numerical Rating Scale (NRS): The patient rates their pain on a scale of 0 to 10, where 0 represents no pain and 10 is the worst pain imaginable.
- Visual Analog Scale (VAS): A ruler graduated from 0 to 10 cm where the patient places a cursor to indicate their level of Pain.
- Simple Verbal Rating Scale (SVR): A series of adjectives (absent, mild, moderate, severe, extremely severe) that are converted into numerical values.
What are the 10 levels of pain?
Pain scales allow for the assessment of pain intensity using several methods. Here are the main levels based on the numerical and visual analog scales:
- 0: No pain
- 1-3: Mild pain
- 3-5: Moderate pain
- 5-7: Severe pain
- 7 and above: Very severe or unbearable pain
These levels may vary slightly depending on the scale used, but they provide a common basis for pain assessment.
What is the VAS pain scale?
The visual analog scale The Visual Analogue Scale (VAS) is a self-assessment tool for pain based on a scale from 0 to 10. Here is how the pain levels are defined: 0-3: Mild pain; 3-5: Moderate pain; 5-7: Severe pain; Greater than 7: Very severe pain. The VAS is simple and reproducible, but it can be difficult for some patients to understand, particularly children, the elderly, or those with visual impairments. What are the 10 degrees of pain? Commonly used pain scales do not precisely define 10 specific degrees, but here are some popular methods:
- Numerical Rating Scale (NRS): Rates pain from 0 (no pain) to 10 (the worst pain imaginable).
- Visual Analog Scale (VAS): A 10 cm line where 0 mm corresponds to no pain and 100 mm to unbearable pain. Values are often converted to millimeters.
- Verbal Rating Scale (VRS): Uses adjectives (none, mild, moderate, severe, extremely severe) converted into numerical values from 0 to 4.



